
What to expect for your delivery?
A lot of my patients ask me “what is my due date?” In France and in England we don’t have the same due date. Important information you can keep in mind: your baby will be considered as premature before 37 weeks and overdue after 41 weeks of amenorrhoea.
What to expect during the different stages of labor?
– 1st stage: early labor
Here we go! You feel the first real uterine contractions. They least 1 minute and are regular, every 5 minutes during, at least, 2 hours, with cervix modifications.
Sometimes, you may have contractions without cervix modifications. It’s a false labor! It is normal and it happens very often. But, no worries, it is not time to go to the hospital!
Your baby could be in different position. The most common is the cephalic presentation (head first).
Some babies are in a breech position. It means your baby is in a bottom-down position. Some others are in a transverse position.
For the last two options, you will probably have a C-section. For the 1st one, if everything else is fine, you will be able to give birth naturally.
The completion of this stage of labor comes when your cervix is fully dilated (about 10 centimetres or 4 inches).
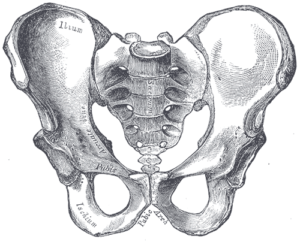
– 2nd stage: Your baby is engaged (thanks to the uterine contractions) when the biggest diameter of his head crosses the brim of the pelvis (it is the highest part of your pelvis) and your cervix is fully dilated.
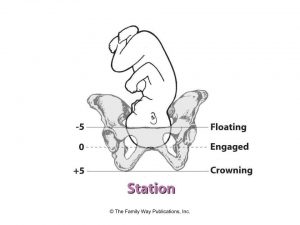
Your baby drops down into your pelvis and you can feel it as he is pushing on your pelvic floor. You will also feel a pushing sensation around your rectum with the sensation you have to start to push.
Some positions will help your baby to go down:
- Hanging position with Swiss ball

- all fours with swiss ball

- Squatting

Don’t hesitate to go walking a little bit as the gravity help your baby.
– 3rd stage: expulsion it is time to push!
It last approximately 30 min (sometimes much longer, it is one of the reason why your pelvic floor and you pelvis are not damaged in the same way from one mother to another).
Maybe the obstetrician will use a catheter to empty your bladder before the delivery.
Ok, so let’s summary! Your baby is engaged through the brim of the pelvis. Now, he is turning his face in front of the sacrum (the bone in your lower back) through the lower brim of the pelvis.
Eventually, the occiput (head bone) of your baby will touch the inferior part of your pubic symphysis. His head is now in a good position and he can come down through the muscle of your posterior pelvic floor (cf article about pelvic floor anatomy).
Every contraction you will have to push to help your baby out. Let’s have a look on the article about breathing exercises during expulsion. It will help you to push correctly and to protect your pelvic floor.
The neck of your baby is pushing on the pubic symphysis and his head come through the anterior perineum. At this point, your midwife can hold it and move his shoulders out with a light rotation.

– 4th stage: Deliverance
Great! Your baby is crying and the midwife holds him. You could think your job is over, but not at all!!
30 min after the delivery of your baby, you will have to expulse your placenta.
If your placenta is not coming out, the midwife will do a placenta removal. It means she will put her hand in the uterus to remove manually the placenta.
It is very painful but essential to avoid infection or even septicemia.
It is normal to loose 500ml of blood during the process. If you bleed more than 500ml, it is called haemoragia and you will need blood transfusion. It happens very often and it is not a big issue. But it also explains why you are so exhausted after the delivery.
What are the different complementary techniques?
The first one is a very controversial: Epidural!
As a French women health physiotherapist, I used to see a lot of delivery with an epidural. But I know some women prefer to give birth naturally without medication and I totally understand it.
There is no good or wrong way. My only advice is: for an epidural you need a good dosage.
It should make your pain a lot more manageable but you should be able to walk around. And you need to keep moving (swiss ball, suspension…).
It is one of the most beautiful moment of life and you should be able to live it fully!
Let’s talk about a difficult topic. Episiotomy!
I know it seems to be an awful thing, but it could save your pelvic floor from a very bad tear (or even an anal tear).
Obviously, it is not systematic and it happens when the anterior part of your pelvic floor is stretched.
During an episiotomy, you midwife cut your pelvic floor; she decide the direction of the cut, avoiding your anal sphincter.
When it tears naturally, there is no control and it could go to your anal sphincter causing a lot more damage and trouble (such as anal incontinence or pelvic pain).
Don’t forget: Perineum massage will limit the risk of tear or episiotomy!
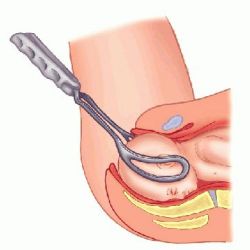
A last technique is the instrumental extraction (ventouse or forceps).
The surgeon will choose to use them
- if the head of your baby is already engaged for a long time causing a fetal distress (anoxia: lack of oxygen).
- Or if the presentation of your baby is not in the right way.
Ventouse or forceps will cut the expulsion off.
Here we are, hope you already know more about giving birth.
Don’t forget to have a look at my others articles about pregnancy and exercises during labor to be prepared for the best time of your life!
Do not hesitate if you have question or you would like me to speak about another topic!



2 Responses
Superb….explained in easy and finest way with duagrams…thank u..
Thank you !